Clinical Data Sources
The Complete Guide to Clinical Data Sources
We’ve spent the last three posts outlining the significant challenges impacting access to clinical data. Now is the time for payers to take on a leadership role in this area.
Consider:
- Value-Based Care contracts present an opportunity to incent providers to move as much data into the EMR with improved standards for data quality and governance as possible.
- Moving away from paper and fax to more structured and digitized data by encounter can increase flow of clinical data into EMRs while reducing the costs required for chart abstraction, third party and HIE fees, and complex translation of unstructured data.
Once it’s captured, the costs and friction of pulling clinical data from diverse EMR environments can be reduced by leveraging emerging legislation on interoperability standards such as FHIR. By promoting these policies and technical innovation, payers can help pave the way for true holistic member records and managing clinical data from an enterprise perspective.
Enterprise view of clinical data
What might this enterprise approach to clinical data look like? By aligning internal initiatives and competencies, payers can scale efficiencies. The following graphic depicts a conceptual view of how it might work to support both operational performance and member engagement goals.
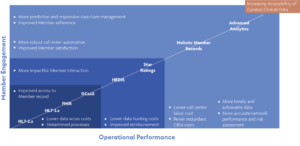
Foundational to this effort is leveraging FHIR standards to enable a more scalable and standardized method of accessing clinical data from source systems. This can reduce the costs of accessing data and streamline internal processes. It’s also required by CMS and establishes the technical underpinnings to improve members’ access to their own health records. This important building block must be coupled with advanced data curation services to ensure that the completeness and accuracy of the data received is as high as possible before being applied to other applications.
Early payoffs of holistic member records
HEDIS® and Stars
As a foundational measurement of quality for payers, HEDIS®1 is an ideal use case for receiving an influx of improved clinical data — especially since it also feeds a subset of Star program measures required by Medicare Advantage. Powered with FHIR and data curation as a service (DCaaS), an enterprise approach to HEDIS® and Stars can help reduce the data-hunting costs associated with reporting requirements, while also improving reimbursement levels by boosting Star ratings. Payers make a further critical step toward a holistic member record by linking these data to other measures like CAHPS and internal CRM data sources.
Improved member service
With more clinical data available, CRM and call center operations can use existing automation solutions to address more member queries. By scaling the capacity to address more clinical queries, call center labor costs may be reduced while member satisfaction scores rise.
More accurate predictive analytics
When clinical data merges with other datasets to form the holistic member record, it enables payer analytics teams to generate more timely and accurate member cohorts to mine for emerging risks. They can then harness that more robust clinical data to improve predictive algorithms and trigger more effective messaging through case and care management. Ideally, they can align more accurate and predictive clinical data with behavioral insight to help improve rates of treatment adherence — which goes a long way in controlling the escalating costs associated with various comorbidities and poly-chronic treatment requirements.
The potential to align technical advances in interoperability and data curation with provider incentives to improve the quality and accessibility of clinical data has never been higher. Payers that realize efficiencies in scale and performance will gain competitive differentiation through more intelligent and responsive member engagement and more scalable, effective and data-driven operations.
1HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).